Vol 129: Rewriting Fate
Natalie was a friend and someone who spent her entire life learning how to coexist with pain. She would have celebrated her birthday in two days. Instead, next month will mark four years since her death in 2022 from complications related to sickle cell disease.
I wrote about Natalie previously in this column. Sudden pain, emergency room visits, missed work, and missed celebrations were rituals in her short life. I remember the exhaustion more than anything else. Not ordinary tiredness, but the kind of physical and emotional fatigue that comes after decades of pain and learning to live beneath the weight and shadow of uncertainty. And although the stability of her health never fully lasted, Natalie remained remarkably hopeful.
She became a physician who advocated for others within the sickle cell community and tried to help patients navigate a disease she herself could never truly escape. At the time of her death, sickle cell disease was a fatal certainty. Today, that certainty no longer feels quite as absolute. That’s because something extraordinary is quietly unfolding in medicine right now and I’m not entirely sure that the public fully appreciates the magnitude of it just yet.
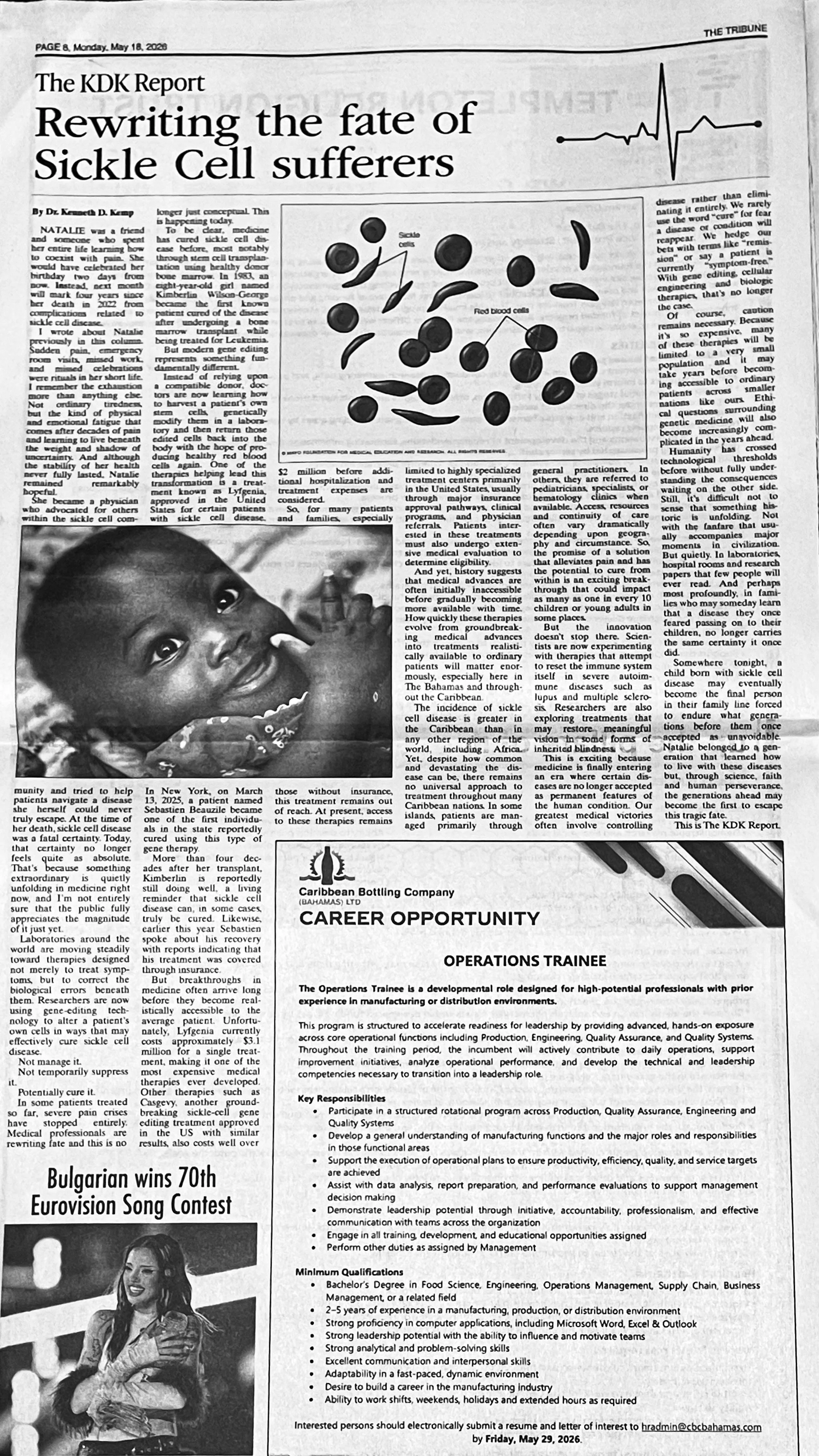
Laboratories around the world are moving steadily toward therapies designed not merely to treat symptoms, but to correct the biological errors beneath them. Researchers are now using gene-editing technology to alter a patient’s own cells in ways that may effectively cure sickle cell disease. Not manage it. Not temporarily suppress it. Potentially cure it. In some patients treated so far, severe pain crises have stopped entirely. Medical professionals are rewriting fate and this is no longer just conceptual. This is happening today.
To be clear, medicine has cured sickle cell disease before, most notably through stem cell transplantation using healthy donor bone marrow. In 1983, an eight-year-old girl named Kimberlin Wilson-George became the first known patient cured of the disease after undergoing a bone marrow transplant while being treated for Leukemia.
But modern gene editing represents something fundamentally different. Instead of relying upon a compatible donor, doctors are now learning how to harvest a patient’s own stem cells, genetically modify them in a laboratory and then return those edited cells back into the body with the hope of producing healthy red blood cells again. One of the therapies helping lead this transformation is a treatment known as Lyfgenia, approved in the United States for certain patients with sickle cell disease. In New York, on March 13, 2025, a patient named Sebastien Beauzile became one of the first individuals in the state reportedly cured using this type of gene therapy.
More than four decades after her transplant, Kimberlin is reportedly still doing well, a living reminder that sickle cell disease can, in some cases, truly be cured. Likewise, earlier this year Sebastien spoke about his recovery with reports indicating that his treatment was covered through insurance.
But breakthroughs in medicine often arrive long before they become realistically accessible to the average patient. Unfortunately, Lyfgenia currently costs approximately $3.1 million for a single treatment, making it one of the most expensive medical therapies ever developed. Other therapies such as Casgevy, another groundbreaking sickle-cell gene editing treatment approved in the US with similar results, also costs well over $2 million before additional hospitalization and treatment expenses are considered.
So, for many patients and families, especially those without insurance, this treatment remains out of reach. At present, access to these therapies remains limited to highly specialized treatment centers primarily in the United States, usually through major insurance approval pathways, clinical programs and physician referrals. Patients interested in these treatments must also undergo extensive medical evaluation to determine eligibility.
And yet, history suggests that medical advances are often initially inaccessible before gradually becoming more available with time. How quickly these therapies evolve from groundbreaking medical advances into treatments realistically available to ordinary patients will matter enormously, especially here in The Bahamas and throughout the Caribbean.
The incidence of sickle cell disease is greater in the Caribbean than in any other region of the world, including Africa. Yet despite how common and devastating the disease can be, there remains no universal approach to treatment throughout many Caribbean nations. In some islands, patients are managed primarily through general practitioners. In others, they are referred to pediatricians, specialists or hematology clinics when available. Access, resources and continuity of care often vary dramatically depending upon geography and circumstance. So, the promise of a solution that alleviates pain and has the potential to cure from within is an exciting breakthrough that could impact as many as one in every 10 children or young adults in some places.
But the innovation doesn’t stop there. Scientists are now experimenting with therapies that attempt to reset the immune system itself in severe autoimmune diseases such as lupus and multiple sclerosis. Researchers are also exploring treatments that may restore meaningful vision in some forms of inherited blindness.
This is exciting because medicine is finally entering an era where certain diseases are no longer accepted as permanent features of the human condition. Our greatest medical victories often involve controlling disease rather than eliminating it entirely. We rarely use the word cure for fear a disease or condition will reappear. We hedge our bets with terms like remission or say a patient is currently symptom-free. With gene editing, cellular engineering and biologic therapies, that’s no longer the case.
Of course, caution remains necessary. Because it’s so expensive, many of these therapies will be limited to a very small population and it may take years before becoming accessible to ordinary patients across smaller nations like ours. Ethical questions surrounding genetic medicine will also become increasingly complicated in the years ahead.
Humanity has crossed technological thresholds before without fully understanding the consequences waiting on the other side. Still, it is difficult not to sense that something historic is unfolding. Not with the fanfare that usually accompanies major moments in civilization. But quietly. In laboratories, hospital rooms and research papers that few people will ever read. And perhaps most profoundly, in families who may someday learn that a disease they once feared passing on to their children, no longer carries the same certainty it once did.
Somewhere tonight, a child born with sickle cell disease may eventually become the final person in their family line forced to endure what generations before them once accepted as unavoidable. Natalie belonged to a generation that learned how to live with these diseases but, through science, faith and human perseverance, the generations ahead may become the first to escape this tragic fate.
This is The KDK Report.